

Abstract
BACKGROUND
The combination of pomalidomide (POM) and dexamethasone (DEX) for the treatment (Tx) of relapsed or refractory multiple myeloma (RRMM) in patients (pts) who have received ≥ 2 prior Tx regimens, including lenalidomide (LEN) and bortezomib (BORT), was approved in Europe in August 2013. POM-DEX is now a standard Tx for pts with RRMM. These pts are at an increased risk for adverse events (AEs) due to prior exposure to multiple lines of Tx and a high disease burden. The European Union post-authorization safety study (EU PASS; NCT02164955) is a prospective, observational, non-interventional study (method: registry) designed to characterize the safety profile of POM-based Tx in pts with RRMM in a real-world setting.
AIM
To report the incidence of key AEs with POM-based Tx, such as neutropenia, thrombocytopenia, venous thromboembolism (VTE), peripheral neuropathy (PN), and second primary malignancies (SPMs), in pts with RRMM treated with POM according to the last prior Tx before starting POM Tx in a post-marketing setting.
METHODS
Pts with symptomatic RRMM initiating POM-based Tx were enrolled at the investigator's discretion. Thromboprophylaxis was administered per local standard practice. AEs were graded according to National Cancer Institute Common Terminology Criteria for Adverse Events (v4.0). The study is ongoing and open for recruitment in centers across Europe. This analysis focused on the safety profile according to the last prior Tx received before starting POM Tx.
RESULTS
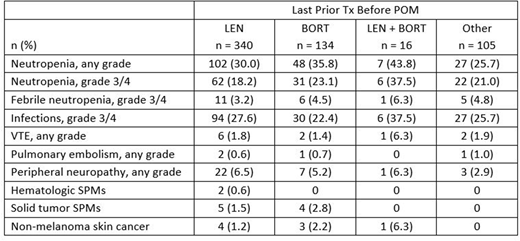
As of July 12, 2018, 596 pts across 100 institutions in 8 European countries were included in the safety population. At the time of data cutoff, Tx was ongoing in 122 pts (20.5%). Median age was 70 yrs (range, 37-92 yrs), with 28.4% of pts aged < 65 yrs, 38.4% between age 65 and 75 yrs, and 33.2% aged ≥ 75 yrs; 54.2% were male. Median time from diagnosis was 4.8 yrs (range, 0.3-26.9 yrs). Median number of prior Txs was 3; 72.1% of pts had ≥ 3 prior lines. Most pts received prior LEN (99.2%) and BORT (99.0%). In 343 pts assessed for Eastern Cooperative Oncology Group performance status (PS), 277 had a PS of 0 or 1 at baseline. Among 595 pts whose prior Tx was entered into the database at the time of data cutoff, the last prior Tx before starting POM was LEN in 340 pts (57.1%), BORT in 134 pts (22.5%), a combination of LEN and BORT in 16 pts (2.7%), and any other drug in 105 pts (17.6%). Tx duration of POM was slightly longer in pts treated with prior BORT than in those treated with prior LEN, with a median Tx duration of 18.7 wks (range, 0.9-150.0 wks) in the LEN group vs 23.7 wks (range, 0.1-148.0 wks) in the BORT group. Across all subgroups, hematologic AEs and infections represented most of all AEs (Table).
CONCLUSIONS
This ongoing, prospective, non-interventional study in pts with RRMM continues to demonstrate that POM-based Tx is generally well tolerated in the real-world setting and that the safety profile is not impacted by the Tx administered immediately before starting a POM-based Tx. Of all pts included in this trial, more pts were treated with LEN immediately before starting POM than any other drug. This analysis shows that AEs are almost similar in pts treated with LEN or BORT or both or any other drug immediately before starting POM Tx. In addition, the reported VTEs, PNs, and SPMs were generally low in all subgroups. Updated data will be presented at the meeting.
Abildgaard:Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Research Funding. Di Raimondo:Celgene: Honoraria; Takeda: Honoraria, Research Funding. Kueenburg:Celgene Corporation: Consultancy, Honoraria. Rosettani:Celgene International: Employment, Equity Ownership. Bacon:Celgene: Employment. Atiba-Davies:Celgene Corporation: Employment, Equity Ownership. Plesner:Janssen: Consultancy; Celgene: Other: Independent Response Assessment Comittee.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal